Ebola Escalation in DRC Highlights Gaps in Global Health Security
The Ebola outbreak in the Democratic Republic of the Congo has surged to become the third largest on record, driven by delayed detection and the absence of targeted vaccines. Experts warn that reduced international funding and the withdrawal of key American health agencies have severely hampered containment efforts, highlighting a critical need for sustained preventive infrastructure over reactive crisis management.
The Democratic Republic of the Congo is currently navigating a severe public health emergency as the Ebola virus continues to expand across the Ituri province. Recent data indicates that the outbreak has reached a critical threshold, ranking among the largest recorded in medical history. Health authorities are now confronting a complex intersection of biological factors, logistical constraints, and shifting geopolitical priorities that threaten to prolong the crisis.
What is driving the rapid escalation of this outbreak?
The initial transmission of the virus occurred well before official recognition, allowing the pathogen to establish a silent foothold within local communities. Medical investigators identified the earliest suspected case on April twenty-fourth, involving a healthcare worker in Bunia. By the time health authorities received formal notification on May fifth, the virus had already claimed the lives of four medical professionals. This initial cluster triggered a rapid investigation, yet the delay proved costly. When international response teams finally arrived on the ground, they encountered a situation that had already expanded to eighty confirmed cases. The window for early containment had effectively closed, forcing responders to shift from prevention to aggressive suppression.
The biological characteristics of the specific viral strain further complicate the situation. This particular outbreak is caused by the Bundibugyo virus, a variant that remains relatively uncommon in modern epidemiological records. Unlike more frequently circulating strains, the Bundibugyo variant lacks established vaccines and widely available therapeutic interventions. Consequently, public health officials cannot rely on immunization campaigns or targeted drug treatments to halt transmission. The response strategy must therefore depend entirely on traditional, labor-intensive methods. Active case finding, strict isolation protocols, and exhaustive contact tracing become the primary mechanisms for breaking the chain of infection.
Geographic and socioeconomic conditions in the affected region create additional barriers to effective containment. The outbreak is unfolding in an area characterized by ongoing armed conflict and significant population mobility. These factors disrupt standard public health operations, making it difficult to maintain consistent surveillance or ensure that isolated patients remain in monitored facilities. Furthermore, the local population faces acute food insecurity and relies heavily on humanitarian assistance networks that are already stretched thin. When communities are struggling to meet basic survival needs, compliance with complex isolation protocols becomes significantly more challenging.
The risk assessment for this outbreak has been continuously updated to reflect its evolving trajectory. National authorities have elevated the threat level to very high, while regional risks remain high and global risks stay low. This tiered classification accurately reflects the current reality. The virus is primarily contained within specific districts of the Democratic Republic of the Congo, yet its capacity for cross-border transmission remains a persistent concern. International health organizations are monitoring neighboring regions closely, particularly Uganda, which has already reported two imported cases. The geographical spread requires coordinated regional strategies rather than isolated national responses.
How does the absence of established treatments complicate containment efforts?
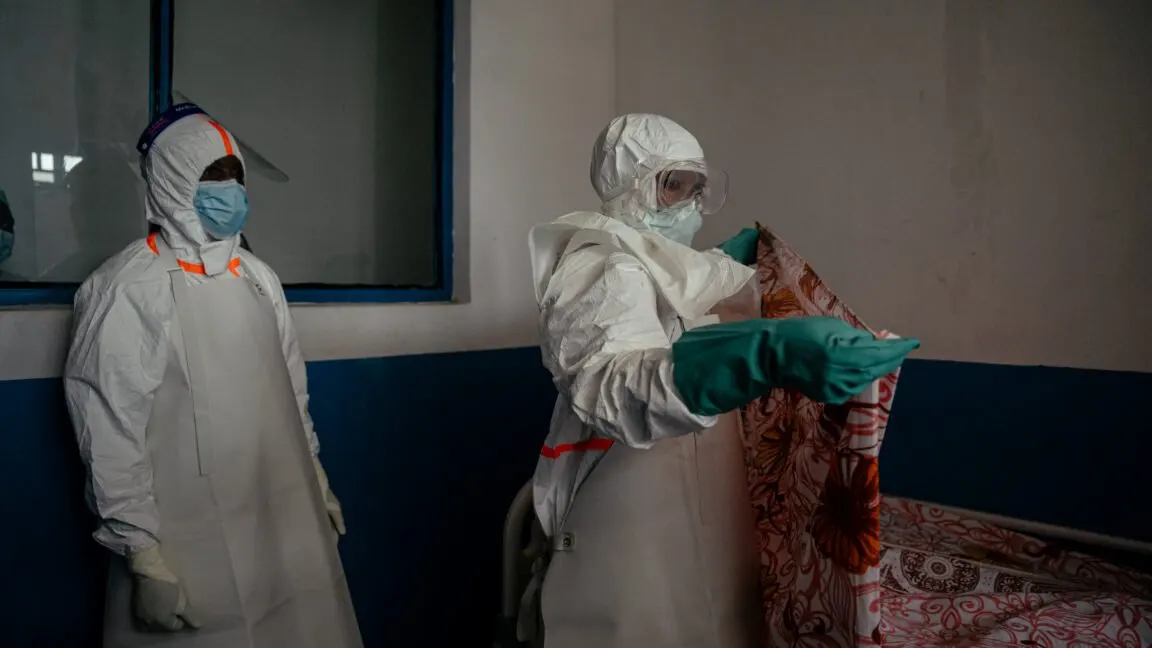
The lack of approved medical countermeasures fundamentally alters the operational tempo of outbreak response. Without a vaccine to create herd immunity or a therapeutic drug to reduce viral load in infected patients, responders must rely on physical barriers and procedural rigor. Personal protective equipment becomes the first line of defense for healthcare workers who treat patients at the most contagious stages of the illness. The absence of adequate stockpiles in the region has left medical staff operating with minimal protection, increasing the risk of nosocomial transmission and further complicating containment efforts.
Contact tracing represents the most critical tool available to epidemiologists in this scenario. Each identified case requires a meticulous investigation to locate everyone who had physical contact with the patient. This process involves documenting daily movements, identifying family members, and monitoring contacts for symptom development over a twenty-one day period. The current operation is tracking approximately one thousand four hundred contacts, a massive undertaking that demands significant manpower and logistical coordination. Any gap in this network can allow the virus to resurge in a new location.
The logistical challenges of sample transport and laboratory diagnostics add another layer of complexity. Early detection relies on rapid testing, yet transporting biological specimens requires strict temperature control to preserve viral integrity. Reports indicate that samples intended for national laboratory analysis were previously managed by international aid organizations. When those support structures are disrupted, the accuracy and speed of diagnostic testing suffer. Delayed results mean delayed isolation, which directly correlates with increased community transmission rates.
Public health infrastructure in the region must also contend with the psychological toll of the outbreak. Healthcare workers face immense pressure while treating patients with a disease that carries a high fatality rate. The emotional burden is compounded by the knowledge that they lack the medical resources available in more developed healthcare systems. Building trust within affected communities requires consistent communication and visible support. When communities perceive that external responders are unable to provide adequate protection or treatment, compliance with public health directives naturally declines.
Why has the withdrawal of major international health agencies altered the response landscape?
The geopolitical landscape surrounding global health security has shifted dramatically in recent years. Historically, certain Western nations served as the primary architects of international disease response frameworks. These countries provided funding, logistical support, and specialized personnel to manage outbreaks in resource-limited regions. However, recent policy decisions have dismantled several key institutions that previously coordinated these efforts. The restructuring of foreign aid agencies and the reduction of domestic public health budgets have created a significant vacuum in global health governance.
The withdrawal from multilateral health organizations has further strained international coordination. When major funding streams are redirected or eliminated, the burden falls disproportionately on the remaining international agencies. These organizations must now stretch limited resources across multiple concurrent crises. The financial strain is evident in the ongoing response to the current outbreak. Health officials have noted that while emergency funding will eventually be allocated, the lack of steady preventive investment leaves national governments vulnerable to sudden surges in disease transmission.
The practical consequences of these policy shifts are already visible on the ground. Medical professionals who previously relied on established supply chains for personal protective equipment now face prolonged shortages. The absence of rapid deployment protocols means that critical resources take weeks to arrive rather than hours. This delay forces healthcare workers to make difficult decisions about patient triage and resource allocation. The cumulative effect is a slower, less effective response that allows the virus to establish deeper roots in affected communities.
International medical experts have publicly criticized the reduction of foreign health assistance. Former officials and epidemiologists have documented how the dismantling of specialized aid programs has directly impacted outbreak management capabilities. The loss of dedicated personnel means that local health ministries must absorb responsibilities that were previously shared. This transition requires time and training that are rarely available during an active crisis. The resulting operational gaps undermine the overall effectiveness of the containment strategy.
What are the long-term implications of shifting from prevention to crisis management?
The current outbreak highlights a fundamental flaw in modern public health strategy. The global health community has historically operated in a cycle of panic and neglect. During periods of relative calm, funding for surveillance, workforce training, and community trust-building is often deprioritized. Resources are then desperately mobilized only after an outbreak reaches critical mass. This reactive approach is inherently inefficient and significantly more costly than maintaining robust preventive infrastructure.
The financial disparity between emergency response and long-term prevention is stark. International leaders have noted that billions of dollars are allocated to military conflicts daily, yet steady funding for disease surveillance is frequently treated as optional. Public health experts argue that consistent investment in national health capacities would prevent outbreaks from reaching explosive growth stages. When communities have reliable diagnostic tools, trained contact tracers, and established communication channels, disease transmission can be contained before it becomes a regional emergency.
The psychological impact on affected populations extends far beyond the immediate health crisis. Communities that experience repeated outbreaks develop a sense of fatalism that undermines future public health initiatives. When residents perceive that external responders only arrive after a crisis has peaked, they are less likely to cooperate with early detection efforts. Building sustainable trust requires consistent presence and transparent communication. This trust is the foundation of effective disease control and cannot be manufactured during an active emergency.
The broader implications for global health security are profound. Disease transmission does not respect national borders, and localized outbreaks can quickly evolve into international threats. The current response efforts are focused on containing the virus within specific districts, yet the underlying systemic vulnerabilities remain unaddressed. Without a fundamental shift toward preventive funding and sustained international cooperation, the global health community will remain trapped in the same reactive cycle. The cost of inaction will inevitably outweigh the investment required for proactive disease management.
Conclusion
The trajectory of this outbreak will ultimately depend on the alignment of political will, financial commitment, and operational execution. Health authorities are currently racing to implement isolation protocols and trace contacts, yet the structural gaps in the global health architecture continue to hinder progress. Sustainable disease control requires more than temporary emergency funding. It demands a permanent commitment to building resilient health systems, training local workforces, and maintaining transparent communication channels. The window for preventing the next surge is open, but it will close quickly if the focus remains solely on suppression rather than systemic reform.
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Wow
0
Wow
0
 Sad
0
Sad
0
 Angry
0
Angry
0
Christopher Holloway is the founder and director of Progressive Robot, a UK-based technology company. A full-stack engineer with more than two decades of experience, he works across PHP development, ecommerce, Linux infrastructure, technical SEO and AI automation, and writes here on technology, AI, hardware and software.








Comments (0)