Kenyan Court Halts US Ebola Quarantine Plan Amid Legal Challenges
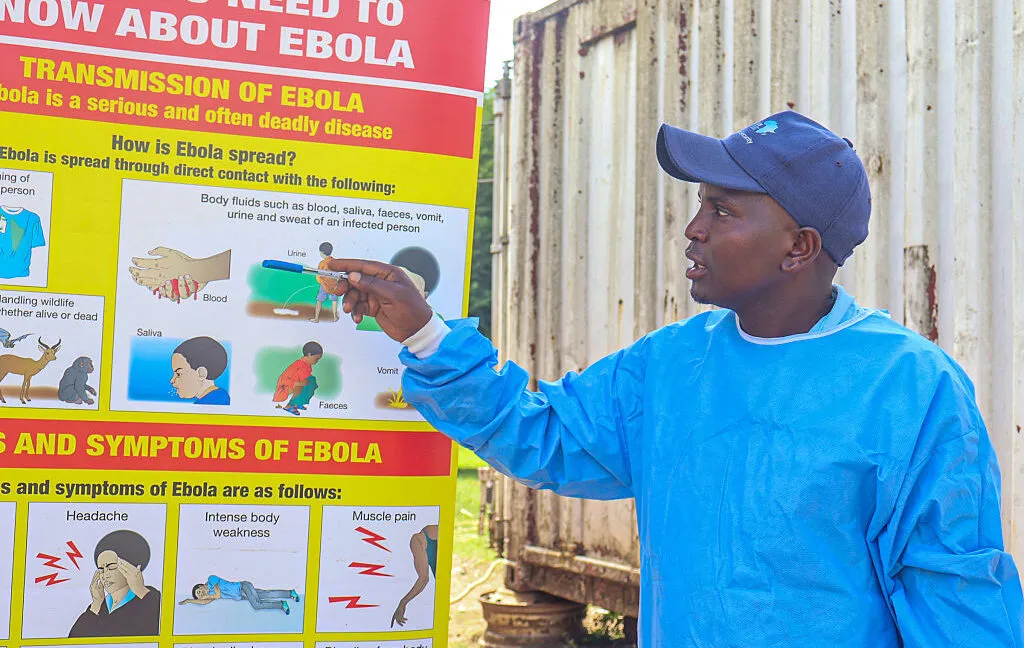
A Kenyan high court has temporarily halted the Trump administration’s plan to establish a makeshift Ebola quarantine facility in Laikipia. The ruling cites constitutional concerns and an imminent threat to public safety, forcing officials to reconsider repatriation strategies for exposed citizens amid an ongoing outbreak in the Democratic Republic of the Congo.
When a foreign government halts the establishment of a temporary medical facility, the intersection of public health logistics, diplomatic relations, and constitutional law becomes immediately apparent. A recent judicial intervention in East Africa has paused a proposed quarantine operation, highlighting the complex legal and ethical frameworks that govern cross-border disease management. The decision underscores how emergency response protocols must navigate sovereign boundaries while balancing national security with international health obligations.
What is the proposed quarantine arrangement in Kenya?
The initial strategy involved constructing a temporary medical infrastructure approximately one hundred twenty miles north of the capital city, situated near an existing American military installation. Planners intended to activate a fifty-bed isolation ward by the end of May, followed by a secondary phase introducing specialized biocontainment units for confirmed infections. This two-tiered approach was designed to separate exposed individuals from those actively displaying symptoms, a standard protocol in infectious disease management. The location was selected primarily for its proximity to established logistical corridors and existing aviation infrastructure. However, the rapid deployment model required navigating complex land-use regulations and environmental assessments that typically demand months of review. Emergency medical facilities of this nature usually require rigorous engineering standards to prevent viral leakage, making the accelerated timeline a subject of intense technical scrutiny. Public health officials must ensure that temporary structures meet the same containment benchmarks as permanent hospitals, particularly when handling highly pathogenic organisms. The logistical framework also depends on reliable supply chains for personal protective equipment, specialized medical gases, and waste sterilization systems. Coordinating these resources across international borders introduces additional layers of bureaucratic coordination.
Engineering standards for temporary biocontainment facilities require rigorous structural integrity and redundant life-support systems. Medical engineers must design ventilation networks that maintain negative pressure differentials across every isolation chamber. These systems rely on continuous power supplies and automated monitoring equipment to detect pressure fluctuations instantly. International medical organizations establish strict guidelines for constructing temporary treatment sites in resource-limited environments. Compliance with these standards ensures that viral particles cannot escape through filtration failures or structural gaps. The accelerated timeline for the proposed Kenyan installation raises technical questions about whether adequate quality assurance protocols can be implemented within the planned schedule. Temporary medical infrastructure often faces logistical hurdles related to material transport and specialized labor availability. Coordinating international medical teams requires extensive credential verification and cultural competency training. These operational complexities demonstrate why permanent health facilities remain the preferred standard for managing highly pathogenic outbreaks.
Diplomatic negotiations regarding foreign medical deployments must align with host-nation sovereignty and international health regulations. When nations propose temporary quarantine sites, they must secure land-use permits, environmental clearances, and municipal approvals. These administrative requirements ensure that local communities are protected from potential biological risks. The Trump administration initially outlined a phased deployment model to manage exposed citizens and confirmed cases separately. This approach mirrors standard epidemiological practices that prioritize patient stratification and resource allocation. However, the compressed timeline for facility activation limited the window for thorough regulatory review. Public health experts emphasize that emergency medical infrastructure cannot compromise long-term safety standards. The proposed Laikipia location offered strategic advantages for aviation logistics, yet it also required extensive coordination with regional authorities. Navigating these diplomatic and technical requirements remains essential for any cross-border health intervention.
Why does the constitutional challenge matter?
Legal advocates initiated a formal petition arguing that the unilateral creation of a foreign medical site bypasses established democratic safeguards. The filing emphasizes that public health interventions must align with constitutional guarantees regarding the right to life, equitable access to medical care, and transparent administrative procedures. Courts typically require governments to demonstrate that emergency measures do not circumvent legislative oversight or public consultation processes. The judicial order explicitly referenced an imminent threat to community safety, mandating a pause until a comprehensive hearing can evaluate the proposed agreement. This legal intervention highlights the tension between executive expediency and institutional accountability during health crises. When foreign governments host temporary medical operations, host nations retain the authority to demand full disclosure of operational terms, liability frameworks, and environmental impact assessments. Transparency ensures that local populations are not inadvertently exposed to novel biological risks. The ruling also reinforces the principle that national security decisions cannot override public health protections without rigorous judicial review. Legal scholars note that emergency powers, while necessary during outbreaks, must remain proportionate and subject to independent oversight. The upcoming hearing will determine whether diplomatic agreements can supersede domestic constitutional requirements.
Administrative law requires that emergency executive actions remain subject to legislative review and judicial oversight. When governments invoke emergency powers to bypass standard procurement and land-use procedures, courts must evaluate whether the measures align with constitutional safeguards. Legal frameworks typically demand that public health interventions prioritize community welfare over administrative convenience. The petition filed by constitutional advocates emphasizes that unilateral decisions regarding foreign medical deployments must undergo transparent public consultation. Democratic institutions rely on parliamentary approval to authorize international agreements that affect domestic populations. Judicial interventions during health crises serve as a necessary check on executive authority, ensuring that emergency measures do not permanently alter legal precedents. The upcoming hearing will examine whether diplomatic negotiations adequately addressed local health infrastructure requirements. Legal scholars argue that transparent administrative processes strengthen public trust during medical emergencies.
Constitutional accountability extends beyond domestic borders when national policies impact foreign communities. Host nations possess the sovereign right to evaluate the safety and legality of proposed medical installations within their territory. The Katiba Institute petitioned for disclosure of the operational terms and preparedness plans, demanding that the Trump administration provide comprehensive documentation. This legal strategy underscores the importance of institutional transparency in public health diplomacy. Courts routinely assess whether emergency declarations justify the suspension of standard administrative procedures. The judicial pause mandates a thorough review of the proposed agreement before any construction or deployment begins. Public health advocates stress that community safety must remain the primary consideration in cross-border medical negotiations. The ruling establishes a precedent that diplomatic expediency cannot override constitutional protections. Future health interventions will likely face similar scrutiny regarding transparency and legislative approval.
How does historical precedent inform current repatriation policies?
Previous American responses to similar viral outbreaks provide a clear baseline for evaluating current logistical decisions. Historical data indicates that the United States has successfully managed a small number of repatriated patients without triggering community transmission. Medical professionals have consistently utilized specialized biocontainment wards designed specifically for high-level pathogen isolation. These facilities employ negative pressure ventilation, redundant filtration systems, and strict personnel decontamination protocols to prevent cross-contamination. One notable domestic case involved a traveler who returned with an active infection, leading to healthcare worker exposure. Both affected staff members were transferred to dedicated national treatment centers and recovered fully, demonstrating the efficacy of established domestic infrastructure. Public health experts emphasize that repatriation decisions should prioritize clinical outcomes over political considerations. The existence of proven domestic treatment networks reduces the necessity for foreign medical arrangements. International health regulations generally encourage treating patients within their home country whenever clinically feasible, as familiar medical teams and established supply chains improve recovery rates. The historical record suggests that well-resourced domestic facilities offer superior long-term care compared to rapidly constructed temporary sites.
The evolution of American infectious disease response protocols reflects decades of clinical research and institutional learning. Early viral outbreaks revealed critical gaps in cross-border medical coordination and patient transport logistics. Subsequent policy reforms established dedicated national treatment networks capable of managing high-risk pathogens safely. These networks rely on specialized medical personnel who undergo rigorous training in viral hemorrhagic fever management. Clinical teams utilize standardized decontamination procedures and advanced respiratory support equipment to maximize patient survival rates. The historical success of domestic repatriation efforts demonstrates the value of maintaining robust national biocontainment capabilities. Public health officials consistently emphasize that clinical outcomes improve when patients receive care within familiar medical systems. The established domestic infrastructure also reduces the logistical burden of transporting vulnerable individuals across international borders. These historical lessons continue to shape modern repatriation guidelines and emergency response planning.
Clinical expertise in managing highly pathogenic viruses requires specialized training and controlled environments. Medical teams must navigate complex infection control protocols while providing intensive care to severely ill patients. The United States has developed extensive experience treating Ebola patients through dedicated national facilities. These centers maintain strict operational standards that minimize the risk of secondary transmission. Historical outcomes consistently show that patients treated within proven domestic networks achieve higher survival rates. Public health authorities prioritize clinical safety over diplomatic convenience when planning repatriation strategies. The current judicial pause has prompted officials to reassess the feasibility of foreign medical deployments. Historical precedent strongly supports utilizing established domestic infrastructure for high-risk viral cases. Future repatriation policies will likely continue to emphasize clinical efficacy and institutional accountability.
What are the broader implications for global health diplomacy?
The ongoing judicial pause has forced diplomatic officials to explore alternative host nations, revealing the fragility of ad hoc medical partnerships. International health organizations continue to monitor the outbreak statistics, which reflect a significant toll on affected communities. Recent reports indicate over one thousand suspected and confirmed cases alongside hundreds of fatalities, underscoring the persistent severity of the regional crisis. Public health analysts observe that unilateral repatriation strategies often strain bilateral relationships and complicate coordinated outbreak responses. When nations prioritize domestic evacuation over regional containment, they risk undermining global health security frameworks. The withdrawal from multilateral health agencies and the restructuring of foreign aid programs have altered how emergency medical resources are distributed worldwide. Experts note that sustainable disease management requires sustained institutional commitment rather than reactive diplomatic maneuvers. The current situation illustrates how domestic policy shifts can ripple through international health networks, affecting both prevention efforts and treatment accessibility. Maintaining transparent communication between host governments and evacuating nations remains essential for preserving trust during medical emergencies.
Institutional restructuring has significantly altered how international health organizations coordinate outbreak responses and distribute medical resources. When multilateral agencies experience funding reductions or operational shifts, global health security frameworks become more vulnerable to disruption. Public health experts note that sustainable disease prevention requires consistent diplomatic engagement and long-term investment in regional medical capacity. The current repatriation debate highlights the challenges of managing cross-border health emergencies without robust multilateral support. Transparent information sharing remains essential for maintaining public confidence during medical crises. Citizens rely on accessible data channels to understand transmission risks and treatment availability. For those navigating complex health information landscapes, exploring traditional search alternatives can provide clearer access to verified medical resources and policy updates. The ongoing judicial proceedings will likely influence future diplomatic approaches to foreign medical deployments. Maintaining open communication between host nations and evacuating governments remains critical for preserving international health cooperation.
Global health security depends on coordinated international efforts rather than isolated national responses. Outbreak management requires sustained investment in regional medical infrastructure and cross-border laboratory networks. The judicial intervention in Kenya demonstrates how domestic legal frameworks can reshape international health diplomacy. Host nations retain the authority to evaluate the safety and legality of proposed medical installations. Diplomatic officials must now navigate complex legal requirements while securing alternative treatment locations. Public health authorities will continue monitoring viral transmission patterns and assessing clinical resource availability. The outcome of this legal proceeding will establish important precedents for future cross-border medical operations. Transparent health policy and institutional accountability remain essential for maintaining global health security.
What is the path forward for repatriation efforts?
The judicial injunction has temporarily suspended the proposed medical deployment, leaving diplomatic channels to negotiate alternative arrangements for exposed citizens. Officials must now balance clinical requirements with legal constraints while monitoring the evolving outbreak conditions. The upcoming hearing will determine whether the proposed facility can proceed under revised agreements or if repatriation strategies must shift entirely. Public health authorities will continue to track viral transmission patterns and assess the adequacy of available treatment options. The outcome of this legal proceeding may establish important precedents for future cross-border health interventions. The resolution of this case will underscore the importance of transparent health policy and international cooperation.
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Wow
0
Wow
0
 Sad
0
Sad
0
 Angry
0
Angry
0
Christopher Holloway is the founder and director of Progressive Robot, a UK-based technology company. A full-stack engineer with more than two decades of experience, he works across PHP development, ecommerce, Linux infrastructure, technical SEO and AI automation, and writes here on technology, AI, hardware and software.









Comments (0)