Ebola Outbreak in DR Congo Sparks Hospital Standoff Over Burial Protocols
Violence erupted at a northeastern hospital in the Democratic Republic of Congo as families demanded the release of deceased relatives for traditional burial, sparking a standoff that required military intervention to contain. The incident reflects broader challenges in managing the seventeenth Ebola outbreak, where cultural mourning practices, absent state infrastructure, and historical distrust of medical personnel complicate standard containment protocols.
A sudden outbreak of violence at a regional medical facility has underscored the profound difficulties facing public health authorities in the Democratic Republic of Congo. When hospital tents were torched during a tense standoff over patient burial protocols, military forces were forced to intervene to restore order. The incident highlights how deep-seated community distrust and traditional mourning customs can rapidly escalate into physical confrontations when handling highly contagious viral hemorrhagic fevers.
What is the current status of the Ebola outbreak in the Democratic Republic of Congo?
The World Health Organization has identified this event as the seventeenth recorded epidemic to strike the vast central African nation. Medical officials are currently tracking a specific variant known as the Bundibugyo strain, which presents unique clinical characteristics compared to other viral hemorrhagic fever classifications. Public health agencies have noted that more than one hundred seventy-seven individuals have succumbed to the illness across multiple affected regions.
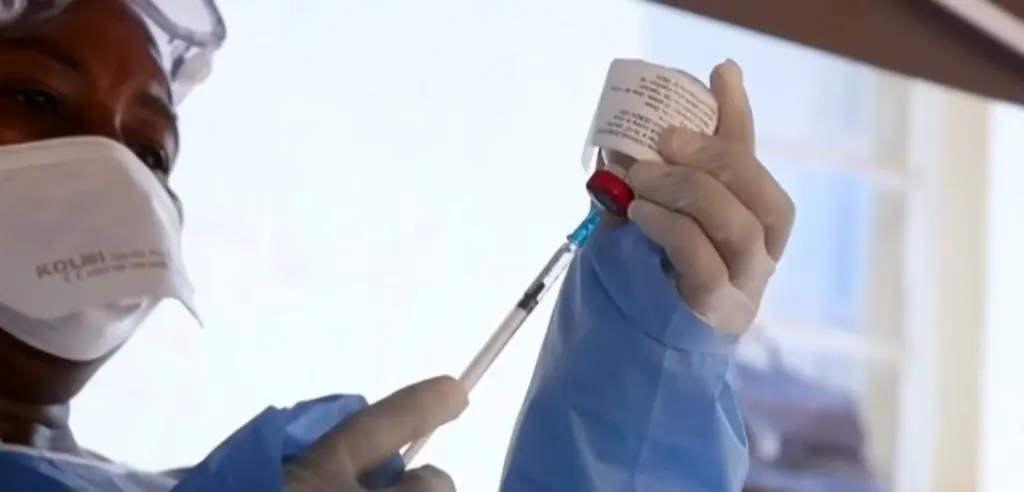
Because no approved vaccine or targeted pharmaceutical treatment exists for this particular strain, containment strategies rely entirely on rigorous precautionary measures and rapid contact tracing networks. Epidemiologists emphasize that the virus spreads through prolonged physical interaction with infected individuals or their bodily fluids. This transmission pathway necessitates strict isolation protocols from the moment of suspected exposure.
Rural healthcare facilities frequently struggle to maintain these boundaries due to limited resources and geographic constraints. The absence of therapeutic interventions forces medical teams to depend on supportive care while simultaneously working to prevent secondary infections within vulnerable communities. Public health officials continue to monitor case progression closely, recognizing that each new cluster requires immediate logistical coordination to halt further viral propagation.
The Incident at Rwampara Hospital
Tensions escalated sharply at the Rwampara medical facility located in the northeastern Ituri province, which serves as a primary epicenter for the current crisis. A confrontation began when hospital administrators refused to release the remains of a twenty-four-year-old deceased patient whose father served in the national military. Families requested immediate custody of the body to conduct customary interment rites, but infection control guidelines strictly prohibit such transfers during active outbreaks.
Medical staff explained that handling uncontained corpses poses an extreme risk to funeral participants and surrounding neighborhoods. The disagreement quickly mobilized a large crowd outside the facility boundaries. Several individuals set fire to the isolation tents designated for active patients, leaving only charred structural remnants behind. A healthcare worker sustained injuries from thrown projectiles during the chaos.
Military units were subsequently deployed to secure the perimeter and disperse the gathering through warning shots. The rapid intervention prevented further property destruction but left deep emotional scars among the waiting relatives. Security personnel eventually facilitated a guarded transfer of three caskets to a designated cemetery site away from the town center.
Why does cultural mourning practice complicate epidemic control?
Traditional burial customs across rural Congolese communities often involve direct physical contact with deceased relatives and extensive communal gatherings. Civil society representatives have documented that mourners frequently embrace corpses, wash remains, and distribute personal clothing items to preserve family memory. These practices hold profound spiritual significance but directly contradict standard viral hemorrhagic fever containment guidelines.
Public health experts note that prolonged exposure to bodily fluids during mourning rituals creates highly efficient transmission pathways for the virus. When large groups assemble for funeral ceremonies without protective barriers, secondary infection clusters emerge rapidly in surrounding villages. Community leaders acknowledge that these cultural obligations cannot be easily abandoned during crisis periods.
Instead, they advocate for modified rites that preserve emotional dignity while eliminating direct contact with remains. Educational campaigns have attempted to explain how viral particles survive on clothing and household surfaces long after death occurs. Despite repeated outreach efforts, historical skepticism toward external medical authorities continues to undermine compliance rates. Many residents view modern infection protocols as unnecessary restrictions rather than essential protective measures.
Bridging this gap requires sustained dialogue between local elders, religious figures, and epidemiological teams to develop culturally acceptable alternatives that still prevent viral spread. Public health initiatives must prioritize community engagement strategies that respect traditional values while enforcing necessary safety boundaries during active transmission periods.
The Burial Process and Community Reaction
Healthcare workers prepared for the interment by donning full personal protective equipment before approaching the caskets. Medical personnel carefully loaded three sealed containers onto a specialized transport cart and moved them toward the cemetery grounds. Families gathered at a distance to witness the proceedings while maintaining strict safety boundaries.
One relative expressed profound grief over being denied final visual contact with his father, noting that the rushed separation caused lasting emotional distress. Another community member openly questioned whether the illness actually existed, describing it as an imaginary condition rather than a documented medical reality. Security escorts accompanied the procession through multiple jeeps filled with armed personnel and law enforcement officers.
Historical records indicate that Congolese security forces have occasionally been accused of exacerbating public suspicion toward medical teams during previous epidemic waves. Some individuals participating in the initial hospital standoff were themselves military affiliates closely connected to the deceased patient. Their involvement complicated efforts to establish neutral ground between grieving families and infection control specialists.
The eventual burial involved hazmat-suited workers spraying disinfectant on the exterior of each coffin before lowering them into prepared graves. A local pastor recited biblical verses while mourners sang traditional dirges in subdued tones, marking a somber conclusion to the day's events. Medical teams documented the procedure carefully to ensure compliance with international safety standards.
How does regional instability affect public health responses?
The Ituri province has experienced decades of limited state service delivery, leaving rural populations without reliable infrastructure for routine healthcare or emergency response. Armed groups operating throughout the restive region have repeatedly conducted massacres that destabilize local governance and disrupt supply chains. Communities increasingly attribute slow epidemic containment to governmental neglect rather than medical inadequacy.
Officials monitoring conditions in nearby Mongbwalu report that residents now recognize the necessity of avoiding physical contact with suspected cases, yet they remain concerned about inadequate facility design. Isolation wards and triage zones have not been properly established across multiple treatment centers. Suspected patients are frequently housed alongside individuals suffering from unrelated illnesses within shared hospital corridors.
This mixing creates elevated infection risks for both vulnerable populations and medical staff attempting to provide care. Public health authorities recognize that structural deficiencies in rural healthcare networks fundamentally undermine outbreak management efforts. Without dedicated containment infrastructure, standard protocols become impossible to execute safely. Long-term solutions require coordinated investment in regional medical facilities, consistent staffing programs, and reliable logistical support for emergency response teams.
Community trust rebuilding depends on demonstrating tangible improvements in service delivery rather than relying solely on temporary crisis interventions. Public health authorities must continue documenting these behavioral shifts to refine outreach methodologies for subsequent outbreaks. Sustainable epidemic control ultimately rests on aligning medical necessity with community dignity while rebuilding trust through reliable service delivery and structural investment in rural healthcare networks.
Conclusion
Managing viral hemorrhagic fevers in conflict-affected regions demands more than clinical expertise and protective equipment. Public health initiatives must address historical grievances, infrastructure deficits, and cultural expectations simultaneously to achieve sustainable containment outcomes. Medical teams operating in remote provinces face relentless pressure from limited resources, geographic isolation, and community skepticism that stems from decades of institutional absence.
Future epidemic responses will require integrated strategies that combine rapid contact tracing with culturally adapted mourning alternatives and permanent healthcare facility upgrades. Security forces can temporarily restore order during violent incidents, but lasting stability depends on consistent government presence and transparent communication about disease progression. Community members who initially resisted isolation protocols gradually adopted safer practices when they witnessed the scale of local transmission firsthand.
Public health authorities must continue documenting these behavioral shifts to refine outreach methodologies for subsequent outbreaks. Sustainable epidemic control ultimately rests on aligning medical necessity with community dignity while rebuilding trust through reliable service delivery and structural investment in rural healthcare networks. Long-term resilience requires coordinated regional planning that prioritizes both clinical safety and cultural respect during future crisis periods.
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Wow
0
Wow
0
 Sad
0
Sad
0
 Angry
0
Angry
0
Christopher Holloway is the founder and director of Progressive Robot, a UK-based technology company. A full-stack engineer with more than two decades of experience, he works across PHP development, ecommerce, Linux infrastructure, technical SEO and AI automation, and writes here on technology, AI, hardware and software.








Comments (0)