US Shifts Ebola Response to Overseas Quarantine and Border Controls
The United States is implementing strict travel restrictions and halting the repatriation of exposed American citizens, opting instead to establish quarantine facilities in Kenya. Public health experts warn that border closures and reduced international cooperation may hinder outbreak containment, while domestic agencies struggle with severe staffing shortages that complicate airport screening efforts. These measures reflect a significant policy shift that prioritizes geographic separation over traditional medical repatriation protocols.
The ongoing Ebola outbreak in the Democratic Republic of the Congo has triggered a significant realignment in American public health strategy, moving away from traditional repatriation protocols toward overseas containment and stringent border controls. As international health agencies mobilize resources to address the rapidly expanding crisis, the United States has implemented a series of measures designed to physically separate the nation from the virus. This approach marks a notable departure from established emergency response frameworks and has sparked extensive debate among epidemiologists and policy analysts regarding its efficacy and ethical implications.
What is driving the shift in American repatriation policy?
Historical precedent for managing infectious disease outbreaks has consistently favored the repatriation of infected or exposed nationals to specialized medical facilities within their home country. The United States previously maintained several high-containment units capable of treating Ebola patients with advanced clinical resources and rigorous safety protocols. However, the current administration has decided to halt these return flights for individuals who have been exposed to the virus or confirmed infected during the ongoing crisis in the Democratic Republic of the Congo.
Instead, officials are working to establish a dedicated quarantine and treatment facility in Kenya, a decision that requires formal approval from Kenyan authorities before implementation. Some members of the United States Public Health Service Commissioned Corps have already received deployment notices to support this overseas effort. The policy shift follows the recent cases of two American medical professionals working as missionaries in the region. Dr. Peter Stafford, who is critically ill with the disease, is receiving care in Germany alongside his family. Another exposed colleague has been placed under monitoring in the Czech Republic. These developments highlight a broader strategic pivot toward geographic separation rather than centralized domestic treatment.
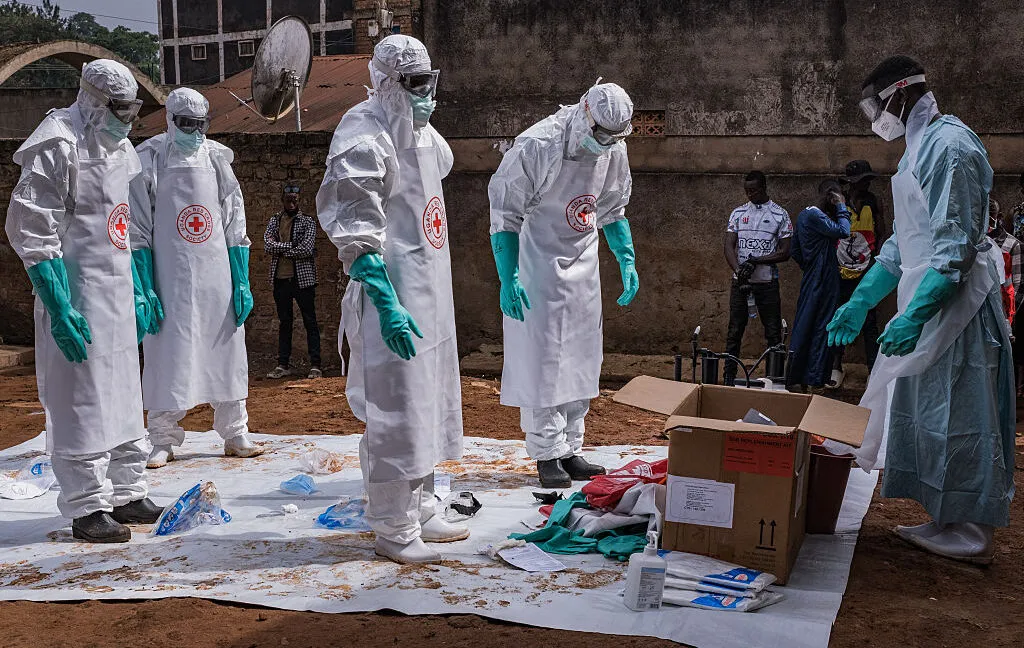
The current crisis involves the Bundibugyo strain of the Ebola virus, which has demonstrated a high fatality rate and rapid transmission pattern in the region. The outbreak was first announced in mid-May and has already become the third largest recorded in history. International health agencies report over one thousand suspected and confirmed cases alongside hundreds of fatalities, though these figures likely represent a significant undercount due to limited testing capacity in remote areas. The speed of the spread has overwhelmed local medical infrastructure, necessitating rapid deployment of isolation units and trained healthcare workers. Managing a strain with such aggressive characteristics requires coordinated logistics and sustained funding, both of which are complicated by shifting national policies. The decision to establish a treatment center in Kenya reflects an attempt to create a regional hub that can serve multiple affected countries simultaneously.
Why do travel restrictions draw criticism from global health experts?
The escalation of border controls has drawn sharp criticism from public health authorities who argue that blanket travel bans rarely improve outbreak containment. International health organizations emphasize that such measures often generate unnecessary fear, disrupt local economies, and discourage transparent reporting from affected regions. When movement is restricted, travelers may instead resort to informal and unmonitored routes, which can inadvertently increase public health risks rather than mitigate them. The current policy bars lawful permanent residents and non-citizens from entering the country if they have visited the Democratic Republic of the Congo, Uganda, or South Sudan within the preceding twenty-one days.
This timeframe aligns with the maximum incubation period for the virus, yet the restriction extends to nations with minimal or zero reported cases. Uganda has documented only seven infections and one fatality, while South Sudan has reported no cases at all. Epidemiologists note that targeted screening and contact tracing remain far more effective than broad geographic exclusions. The focus on physical separation reflects a political calculation that prioritizes domestic visibility over collaborative disease management, even as global health agencies continue to advocate for coordinated international responses.
Public health researchers have long documented the unintended consequences of restrictive border policies during infectious disease emergencies. When governments implement sweeping travel bans, they often disrupt the very supply chains and humanitarian networks required to contain outbreaks. Medical personnel, diagnostic equipment, and therapeutic supplies face additional delays at checkpoints, slowing down the deployment of critical resources. Furthermore, the stigma associated with geographic restrictions can discourage affected communities from reporting symptoms or seeking treatment, allowing the virus to spread undetected in rural and underserved areas. The current policy extends restrictions to countries with negligible transmission rates, which raises questions about the scientific basis for the geographic scope.
How does the CDC manage screening amid staffing shortages?
The Centers for Disease Control and Prevention is attempting to strengthen airport screening protocols to detect potential cases among arriving travelers, but the agency faces severe operational constraints. The organization currently operates without a permanent director and has experienced significant reductions in senior leadership positions due to budget cuts and organizational restructuring. These staffing gaps have made it difficult to assign sufficient personnel to conduct temperature checks and health questionnaires at major entry points. Jay Bhattacharya, who is currently overseeing the agency, recently circulated an internal message requesting that staff members volunteer for screening duties.
The directive explicitly noted that volunteers could come from any pay grade, underscoring the urgency of the situation. Manual screening procedures require trained individuals to monitor vital signs, review travel histories, and administer preliminary health assessments. Without adequate personnel, the effectiveness of these measures diminishes considerably. The reliance on voluntary labor highlights a broader systemic challenge within federal health agencies during periods of political interference and resource depletion. Effective outbreak response depends heavily on institutional capacity, and the current staffing limitations threaten to undermine even the most well-intentioned screening initiatives.
The operational challenges facing the Centers for Disease Control and Prevention extend beyond immediate staffing shortages and reflect deeper structural vulnerabilities within federal health institutions. Historically, the agency has relied on a stable workforce of epidemiologists, laboratory technicians, and field coordinators to maintain continuous surveillance capabilities. Budget reductions and leadership vacancies have disrupted this continuity, forcing remaining employees to assume multiple responsibilities simultaneously. The request for volunteers to conduct airport screenings illustrates how institutional capacity can be stretched beyond sustainable limits during periods of administrative transition. Temperature checks and health questionnaires require consistent application and accurate documentation to be effective. Inconsistent screening protocols can create false security, allowing asymptomatic carriers to enter the country without proper follow-up. The agency must balance immediate crisis response with long-term workforce development to prevent future operational failures.
What are the long-term implications for international disease surveillance?
The United States withdrawal from the World Health Organization last year has fundamentally altered the architecture of global disease monitoring and emergency response coordination. By severing official ties with the international health body, the country has cut off access to real-time epidemiological data and discontinued financial contributions that support worldwide outbreak preparedness. The loss of funding has forced the organization to reduce its operational staff and scale back essential programs across multiple regions. Furthermore, recent reports indicate that the administration has restricted American scientists from communicating with World Health Organization counterparts, even during concurrent health emergencies such as a hantavirus outbreak on a cruise ship and the ongoing Ebola crisis.
Multinational coordination relies heavily on shared data, joint research initiatives, and unified public health messaging. When major nations disengage from these collaborative frameworks, response efforts become fragmented and less efficient. The current outbreak in the Democratic Republic of the Congo has already surpassed three thousand cases according to preliminary estimates, making international cooperation indispensable. The decision to isolate domestic response mechanisms from global networks may yield short-term political benefits, but it risks weakening long-term pandemic preparedness and delaying critical medical interventions.
The withdrawal from the World Health Organization has created significant gaps in global disease monitoring networks that extend far beyond current outbreak responses. International health surveillance depends on standardized reporting mechanisms, shared genomic sequencing data, and coordinated research funding to track viral mutations and develop targeted interventions. When major economies disengage from these collaborative systems, the remaining member states must absorb additional financial and administrative burdens. The reduction in organizational staff has limited the agency's ability to deploy rapid response teams, distribute medical countermeasures, and coordinate cross-border containment strategies. Scientific exchange between American researchers and international counterparts has historically accelerated vaccine development and treatment optimization. Restricting these interactions delays critical knowledge transfer and fragments the global scientific community. The long-term consequence of reduced cooperation may be a slower response to future pandemics and diminished capacity to prevent cross-border disease transmission.
What is the current status of the Ebola outbreak in the Democratic Republic of the Congo?
The outbreak involves the Bundibugyo strain and has become the third largest recorded, with international health agencies reporting over one thousand suspected and confirmed cases alongside hundreds of fatalities, though actual numbers are likely higher due to limited testing in remote areas.
Why are public health experts criticizing the new travel restrictions?
Experts argue that blanket border closures generate fear, disrupt supply chains, discourage transparent reporting, and divert travelers to unmonitored routes, making targeted screening and contact tracing far more effective for outbreak containment.
How is the CDC addressing airport screening despite leadership vacancies?
The agency is requesting that staff members from any pay grade volunteer to conduct temperature checks and health questionnaires, as budget cuts and organizational restructuring have severely limited available personnel for mandatory screening duties.
What impact has the US withdrawal from the World Health Organization had on global health monitoring?
The withdrawal has severed access to real-time epidemiological data, ended financial contributions, forced staff reductions, and restricted scientific communication between American researchers and international counterparts, fragmenting coordinated pandemic preparedness efforts.
Conclusion
The intersection of domestic policy decisions and global health dynamics reveals a complex landscape where political priorities often diverge from epidemiological best practices. Establishing overseas treatment facilities and enforcing strict border controls may provide a sense of immediate security, yet these measures do not address the underlying mechanisms of viral transmission or the necessity of coordinated international response. Public health professionals continue to emphasize that sustainable outbreak management requires transparent data sharing, robust institutional staffing, and collaborative diplomatic engagement. As the crisis evolves, the effectiveness of these strategies will depend on how well they align with established scientific principles and the practical realities of managing highly contagious pathogens across borders. The coming months will likely determine whether isolated containment efforts can successfully complement global health initiatives or if they will further complicate the path toward widespread disease control.
The evolving response to the Democratic Republic of the Congo outbreak demonstrates how domestic policy choices directly impact global health security. While border controls and overseas treatment facilities may offer immediate political reassurance, they do not replace the foundational requirements of effective epidemic management. Sustainable disease control depends on transparent data sharing, well-funded public health institutions, and sustained international partnerships. The current approach highlights a tension between national isolation and collaborative crisis response, a dynamic that will likely shape future emergency preparedness strategies. As health officials navigate these complex decisions, the focus must remain on evidence-based interventions that prioritize both domestic safety and global health stability. The outcomes of this crisis will inform how nations balance sovereignty with shared responsibility in an increasingly interconnected world.
What's Your Reaction?
 Like
0
Like
0
 Dislike
0
Dislike
0
 Love
0
Love
0
 Funny
0
Funny
0
 Wow
0
Wow
0
 Sad
0
Sad
0
 Angry
0
Angry
0
Christopher Holloway is the founder and director of Progressive Robot, a UK-based technology company. A full-stack engineer with more than two decades of experience, he works across PHP development, ecommerce, Linux infrastructure, technical SEO and AI automation, and writes here on technology, AI, hardware and software.








Comments (0)